
Genuine Facts About Omicron, Delta, Naturally Acquired Immunity, and Vaccines
By James D. Agresti
January 5, 2022
Overview
Given the recent outbreak of the Omicron variant and much still unknown about it, the facts surrounding the Delta variant provide a cautionary tale of how misinformation about SARS-CoV-2 variants provides cover for people who have caused widespread harm and countless deaths.
Government officials and media outlets have often blamed the Delta variant—and are preemptively blaming the Omicron variant—for:
- surging Covid-19 hospitalizations and deaths amid rising vaccination rates and booster shots (President Biden & the New York Times).
- Covid-19 outbreaks in schools (the CDC & WebMD).
- inflation (the Washington Post & the New York Times).
- supply chain disruptions (NPR & the Washington Post).
- sagging economic growth (Reuters & Yahoo Finance).
- “a lot of the problems with the economy” (CNN).
While the Delta variant is much more transmissible than earlier SARS-CoV-2 variants, its mutations don’t materially compromise the naturally acquired immunity that develops when people catch and recover from Covid-19. Though mass media has led people to believe just the opposite, at least 20 studies conducted throughout the pandemic have found evidence that such immunity is potent and lasting.
In contrast, the current crop of Covid-19 vaccines initially provide strong immunity against Delta and earlier variants, but this appears to start waning a few months after vaccination and drops dramatically by six months. The exact reasons for this are not yet proven, but three major possibilities rooted in empirical facts include the following:
- The vaccines are injected into muscles, which produces little-to-no immunity in the upper respiratory tract where the SARS-CoV-2 virus first infects people.
- The vaccines target only one area of the virus called the “Spike protein,” while naturally acquired immunity targets the entire virus.
- The vaccines trigger an immune reaction to only a few Spike variants, while natural naturally acquired immunity attacks a diverse array of Spike variants.
Data and studies on the Omicron variant are just beginning to pour in, but genetic and immunological research suggests Omicron will be more of the same but with greater transmissibility, a lower death rate, and faster vaccine waning. In other words, it seems ideally suited to mitigation via naturally acquired immunity.
However, the higher transmissibility of Omicron requires much better measures to protect people who are highly vulnerable to C-19. This has been a staggering failure of the authorities responsible for C-19 policies.
Taken together, the thoroughly documented facts below show that the horrors commonly blamed on variants are ultimately due to inept policies and actions. Yet, policymakers and public opinion shapers are failing to learn from their errors and continuing down the same destructive paths.
Ph.D. biostatician Dr. Rodney X. Sturdivant, the Director of the Statistical Consulting Center at Baylor University, critically assessed this research and stated, “People will learn more about Covid immunity and vaccines from this article than if they watched and read everything published by most major media outlets since the outset of the pandemic.”
Mutations & Naturally Acquired Immunity
During the very first week of the Covid-19 pandemic in March 2020, a molecular biology journal reported that the SARS-CoV-2 virus that causes Covid-19 “does not mutate rapidly for an RNA virus because, unusually for this category, it has a proof-reading function” in its genome. Throughout the pandemic, science journals have repeatedly confirmed this profoundly important fact.
However, the vast bulk of media outlets have never mentioned it, and U.S. government agencies have virtually ignored it except on a website that stores copies of academic papers.
The upshot of this genetic proof-reading mechanism, as explained in the March 2020 paper, is that once a vaccine for C-19 is developed, it “would not need regular updates, unlike seasonal influenza vaccines.” Implicit in this statement is that the vaccine would trigger a broad immune response that mimics naturally acquired immunity. This involves more than just a few types of antibodies but a diverse array of antibodies, B cells, and two types of T-cells called CD4+ and CD8+.
Such is the case with a wide variety of vaccines for diseases like rubella, mumps, measles, polio, smallpox, and yellow fever. Like naturally acquired immunity, these vaccines commonly provide lifelong protection against these diseases.
Short-lived immunity, on the other hand, typically occurs with diseases like the common cold and flu because the viruses that cause them mutate quickly. As explained in the Journal of Infectious Diseases, “all viruses mutate, but influenza remains highly unusual among infectious diseases” because it mutates very rapidly, and thus, “new vaccines are needed almost every year” to protect against it.
Even still, naturally acquired immunity against strains of the flu can be lifelong. For a remarkable example, a study published by the journal Nature in 2008 found that survivors of the 1918 flu pandemic still had immune B-cells that actively produce “highly functional, virus-neutralizing antibodies” that guard against this disease roughly 90 years later. Moreover, scientists were able to extract these B cells from the subjects’ blood and use them to generate monoclonal antibodies, which had “exceptional virus-neutralizing potency and protected mice from lethal infection.”
As expected for a virus with a genetic proofreading mechanism, at least 20 studies have found evidence that naturally acquired immunity to SARS-CoV-2 is potent and durable. These studies span from early in the pandemic all the way up through the period of Delta variant dominance:
- In May 2020, the South Korean CDC published a study of 285 people who contracted C-19, recovered, and then tested positive again. Contrary to the assumption that they must have caught the disease a second time, viral culture testing was performed on 108 of the subjects, and “all had negative results.” Also, “no case was found” in which someone “was newly infected solely from contact with” one of the people. These facts indicate that the positive C-19 tests were caused by remnants of dead or harmless virus particles. Thus, South Korea changed its policy to treat such individuals as non-infectious.
- In August 2020, the journal Cell published a study of the immune system responses of 206 people in Sweden who had contracted C-19. Unlike other studies that only tested for antibodies, this one measured “T cells,” which are the body’s main source of “long-term immune protection.” This is important because antibodies quickly wane after infections, while T cells provide lasting immunity. The study found that:
- 100% of the subjects who had severe C-19 and 87% who had mild C-19 had “highly functional memory T cell responses, suggesting that natural exposure or infection may prevent recurrent episodes of severe Covid-19.”
- “In line with these observations, none of the convalescent individuals in this study, including those with previous mild disease, have experienced further episodes of Covid-19.”
- In August 2020, after Covid-19 had impacted “over 23 million patients with more than 0.8 million deaths in over 200 countries,” the journal Clinical Infectious Diseases reported the first proven case of someone catching C-19 and then catching it again. This sometimes occurs with all infectious diseases because immunity is not an all-or-nothing phenomenon, and it can be compromised by factors like poor general health, obesity, immunosuppressing drugs, a lack of sleep, or old age. This is one of the main reasons why it is important to reach herd immunity so that C-19 dwindles to the point where it can’t easily spread.
- In October 2020, the International Journal of Infectious Diseases published a study of 804 Covid-19 patients discharged from two hospitals in Italy. It found that two months later, “none has died and none has had any signs of recurrence of infectious at both telephone interview and clinical visit.”
- In November 2020, the journal Cell published a study of 15 people who recovered from mild cases of C-19 to determine if their immune systems developed “a multilayered defense that lasts.” The study found that all of them did, as evidenced by the presence of C-19-specific T cells and B cells in their blood. Both are sources of long-term immune protection. Researchers also tested the cells and found that they reacted appropriately when exposed to the virus that causes C-19. Those results, as the authors point out, are consistent with the fact that no one who previously had C-19 caught it again during major outbreaks on a fishing vessel and at an overnight camp.
- In December 2020, the New England Journal of Medicine published a study that analyzed six months of SAR-CoV-2 infections at four U.K. hospitals among 1,265 staff who already were previously infected with the virus. The study found that only two of these staffers tested positive for C-19 again, and both were asymptomatic.
- In December 2020, the Journal of Infection published a study of 1,038 U.K. healthcare workers who were diagnosed with C-19 in the first wave of the pandemic. During the second wave that began about seven months later, 128 of the same people were tested for C-19 because they showed symptoms of it, but the tests found that none of them had actually caught C-19 again.
- In January 2021 the journal Science published a study of 188 people in the U.S. who contracted Covid-19, most with “mild” cases. The study found that 5 to 8 months later, 95% of them had at least three components of long-term immunity to the disease, such as B cells and T cells. In the words of Shane Crotty, a Ph.D. molecular biologist and coauthor of the paper, “There was a lot of concern originally that this virus might not induce much memory. Instead, the immune memory looks quite good.”
- In February 2021, the European Journal of Clinical Investigation published a paper analyzing all reported cases of C-19 in Austria during the first two waves of the pandemic. It found that people who caught C-19 during the first wave developed a degree of immune protection to the second wave “comparable with the highest available estimates on vaccine efficacies.” The study also found that no one who recovered from C-19 in the first wave died from it during the second wave.
- In February 2021, the journal Cell published a study that reported:
- “it is highly unlikely that SARS-CoV-2 mutations would escape T cell immunity” because the T cells produced by natural infection attack “a very broad array” of areas on the SARS-CoV-2 virus.
- “SARS-CoV-2 mutations exist that could affect” the ability of antibodies to attack certain parts of the virus, but humans produce a “broad range of SARS-CoV-2 neutralizing antibodies” that attack many other parts of the virus.
- “it is unlikely that the virus will be able to evolve escape variants that avoid the majority of humoral and cellular immune memory in Covid-19 cases or Covid-19 vaccine recipients soon.”
- In May 2021, the journal EClinicalMedicine published a study of 43,044 people who were infected with SARS-CoV-2 in the nation of Qatar from April through December 2020. It found that:
- previous infection reduced the odds of contracting C-19 by 94% to 96%.
- none of the reinfections “were critical or fatal.”
- the data “did not show any evidence of waning of immunity for over seven months of follow-up.”
- In May 2021, the journal Clinical Infectious Diseases published a study of 498 people in Switzerland who had Covid-19 during the spring of 2020 and were monitored through January 2021. It found that previous infection reduced the odds of contracting Covid-19 by 86% to 98% for the length of the study “lasting at least 8 months.”
- In June 2021, the journal Nature published a study of 63 vaccinated and unvaccinated people who recovered from Covid-19 and were monitored for a year thereafter. It found that “in the absence of vaccination,” the subjects developed B cells that remained “relatively stable” in number and actually developed “increasing potency and breadth” during “6 and 12 months after infection.” In the words of the paper, these findings “suggest that immunity in convalescent individuals will be very long lasting” and provide protection “against a wide group of variants.”
- In July 2021, the journal Cell Reports Medicine published an “in-depth longitudinal study” of 254 Covid-19 patients who were monitored for up to eight months after infection. It found that “most convalescent COVID-19 patients mount durable antibodies, B cells, and T cells specific for SARS-CoV-2 up to 250 days, and the kinetics of these responses provide an early indication for a favorable course ahead to achieve long-lived immunity.”
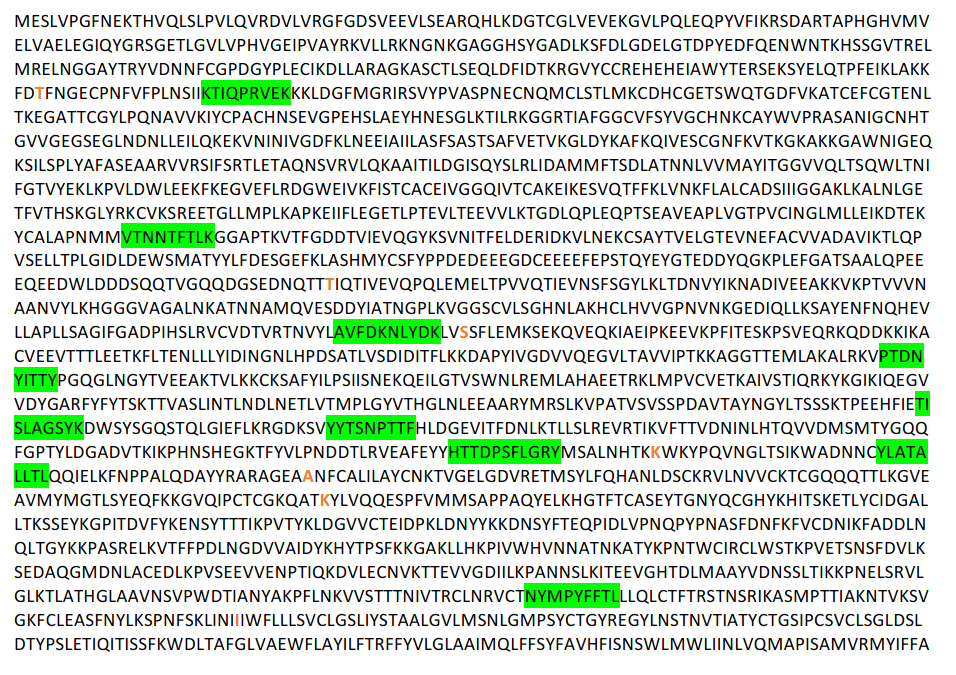
- In July 2021, the journal Open Forum Infectious Diseases published a study that mapped all 45 mutations found in the “3 most prominent global SARS-CoV-2 variants”—namely, Alpha, Beta, and Gamma. It then compared these to a map of 52 areas of the virus attacked by immune CD8+ T-cells found in 30 people who caught and recovered from Covid-19 before the emergence of these variants. The study found that “only 1 mutation” was located in the areas attacked by the T cells, “suggesting that virtually all anti-SARS-CoV-2 CD8+ T-cell responses should recognize these newly described variants.” An appendix to the study provides the entire map, a typical section of which is shown below with the areas attacked by the T cells in green highlighting and the mutations in orange:

- In July 2021, the journal Cell Reports Medicine published a more expansive study that mapped all mutations found in the United Kingdom (Alpha) variant, the South Africa (Beta) variant, the Brazil (Gamma) variant, and the California (Epsilon) variant. It then compared these to a map of the areas of the virus attacked by immune CD4+ and CD8+ T-cells found in 28 people who caught and recovered from Covid-19 before the emergence of these variants. The study found that:
- “the T cell responses against SARS-CoV-2 are highly” diverse, “with tens of different” areas on the virus attacked by “CD4+ and CD8+ T cells in a given individual.”
- 93% of 280 areas attacked by CD4+ cells and 97% of 523 areas attacked by CD8+ cells “are unaffected by mutations found in all of the different variants.”
- “a similar pattern is observed when the magnitude of T cell responses associated with the various” areas “is considered, rather than the simple number of” areas.
- “even in the” areas “affected by single mutations, no negative effect on the predicted” ability of the T-cells to attack the virus “in the majority of cases is expected.”
- T cells “may contribute to limiting Covid-19 severity induced by VOCs [variants of concern] that partially or largely escape neutralizing antibodies.”
- In August 2021, the European Journal of Internal Medicine published a study of 4,276 hospital employees during an “unprecedented surge in SARS-CoV-2 infections driven by the Delta variant” in India during April/May 2021. It found that “previous infections with SARS-CoV-2 were significantly protective against all studied outcomes, with an effectiveness of 93% (87 to 96%) seen against symptomatic infections, 89% (57 to 97%) against moderate to severe disease and 85% (-9 to 98%) against supplemental oxygen therapy. All deaths occurred in previously uninfected individuals. This was higher protection than that offered by single or double dose” of AstraZeneca’s Covid-19 vaccine.
- In August 2021, the journal Science published a study of antibodies found in the blood of four people who had “mild to moderate” cases of Covid-19 before the emergence of the Alpha, Beta, Gamma, and Delta variants. It found that “highly potent neutralizing antibodies with activity against” all of those variants “was present in at least three of four” subjects.
- In November 2021, the New England Journal of Medicine published a study of 353,326 people in Qatar who had been infected with C-19 from February 2020 through April 2021 while the Alpha and Beta variants were circulating. The study found “no cases of critical disease” and “no cases of death” among any of the people who were previously infected.
- In December 2021, the journal Healthy Longevity published a study of 1,377 nursing home residents and staff in England who were infected with Covid-19 from April 10 to August 3, 2020 before the emergence of the Alpha variant. The study monitored them through January 2021 when “the Alpha variant accounted for more than 90% of all cases in England.” It found that previous infection reduced the odds of catching C-19 by 94–97% for staffers and 96–98% for residents “even in the high-risk, closed environment of care homes and after the emergence of the Alpha variant, consistent with our previous observations and those of others.”
The studies above are not cherry-picked exceptions from a larger pool of studies that found otherwise. They are the rule, as proven by systematic reviews in medical journals:
- In May 2021, the journal Reviews in Medical Virology published “the first systematic review to synthesize the evidence on the risk of SARS-CoV-2 reinfection over time.” It found that “reinfection was an uncommon event (absolute rate 0%–1.1%), with no study reporting an increase in the risk of reinfection over time.”
- In September 2021, the journal Evaluation & the Health Professions published a “systematic review” of studies that “estimate the risk of SARS-CoV-2 reinfection among those previously infected with SARS-CoV-2.” Based on 10 studies that met the inclusion criteria, the authors found that “the protective effect of prior SARS-CoV-2 infection on re-infection is high and similar to the protective effect of vaccination.” These studies “included 9,930,470 individuals with a median observation period that ranged from one to 10.3 months.”
- In November 2021, the journal Infectious Diseases published an analysis of “well conducted biological studies” about naturally acquired immunity in a massive biomedical research database. It found that “multiple epidemiological and clinical studies, including studies during the recent period of predominantly delta … variant transmission, found that the risk of repeat SARS-CoV-2 infection decreased by 80.5–100% among those who had had Covid-19 previously.”
Because it is practically impossible to conduct a “gold standard” randomized controlled trial for naturally acquired immunity, no studies on this matter are totally conclusive. Nevertheless, a broad spectrum of studies with varying methodologies indicate that infection and recovery from Covid-19 produces robust and lasting immunity in the vast majority of people.
Importantly, naturally acquired immunity can only be as strong as each person’s immune system, and the same applies to vaccines. Vaccines don’t directly attack virulent microbes in the same manner as antibiotics or anti-viral medicines. Instead, they trigger people’s immune systems to react more quickly than usual and kill pathogens before they can do harm.
So if a person’s immune system is weakened by a serious medical condition or factors as common as poor sleep, excessive alcohol, psychological stress, obesity, or old age, their “immunity” can fail to protect them.
Nor is “immunity” an all-or-nothing phenomenon. In fact, scientific journals draw important distinctions between different types of immunity, such as:
- “clinical immunity,” defined by a 2009 paper in the journal PLoS as an immunity that “reduces the probability that an individual will develop clinical disease.” Notably, this doesn’t prevent infections but limits their harmful impacts by killing the pathogens before they do serious harm.
- “sterilizing immunity,” defined by a 2016 paper in the journal Scientific Reports as “a unique immune status, which prevents effective virus infection into the host.” The paper emphasizes that this is “different from” clinical immunity that “allows infection but with subsequent successful eradication of the virus.”
- “upper respiratory tract immunity,” which prevents pathogens from reproducing in the nasal passages and throat—as opposed to merely in the lungs. As explained in a 2020 paper in the journal Infection and Immunity, this is vitally important because:
- “the upper respiratory tract is both the initial site of infection and the major locale for antibody” production after respiratory infections.
- “there is a fundamental difference in immune and inflammatory responses generated in the upper and lower respiratory tracts.”
- the “optimal approach” for disease prevention is to generate immune “responses in both the upper and lower respiratory tracts,” as occurs with natural infection.
And within each type of immunity are varying levels of it. For example, a 2004 paper in the journal Immunological Reviews notes that people who are “clinically immune” to malaria have “variable levels of immunity” that tend to increase each time a person is exposed to the parasites that cause the disease.
Given the biological fact that SARS-CoV-2 has a proofreading mechanism in its genome, it should come as no surprise that its mutations and variants have not had a material impact on naturally acquired immunity. Again, this was predictable and predicted during the first week of the pandemic.
Nonetheless, the vast bulk of media outlets and government officials have been silent about those vitally important facts while fostering the opposite impression by blaming the Delta variant for mounting Covid-19 deaths and making statements like these:
- ABC News (6/24/20) quoting Anthony Fauci (6/8/20): People who contract Covid-19 don’t have “a uniformly robust antibody response, which may be a reason why, when you look at the history of the common coronaviruses that cause the common cold, the reports in the literature are that the durability of immunity that’s protective ranges from 3 to 6 months to almost always less than a year.”
- The Guardian (7/12/20): “People who have recovered from Covid-19 may lose their immunity to the disease within months, according to research suggesting the virus could reinfect people year after year, like common colds.”
- CNBC (7/13/20): “World Health Organization officials said Monday that patients who recover from Covid-19 may be able to get the coronavirus again, adding that studies suggest their immunity may wane after a few months.”
- Fox 5 New York (7/13/20): “A study published on July 11 by researchers at King’s College London found that antibodies detected in the human body which fight the coronavirus declined after just a few weeks, leaving the possibility of herd immunity out of the question.”
- The Center for Infectious Disease Research and Policy at the University of Minnesota, reporting on studies published in the New England Journal of Medicine and the journal Nature (7/22/20): “Mounting evidence of fleeting immune response” to Covid-19 has been found by studies “showing rapidly decreasing antibody levels after infection” and “dim hopes” for allowing “recovered Covid-19 patients to return to work or travel.”
The fatal flaw in those statements is that antibody levels fall after all types of infections and are not a measure of long-term immunity. Condensing extensive research on this subject published by the journal Nature in May 2021, Dr. Ali Ellebedy (the primary author) plainly stated:
Last fall, there were reports that antibodies wane quickly after infection with the virus that causes Covid-19, and mainstream media interpreted that to mean that immunity was not long-lived. But that’s a misinterpretation of the data. It’s normal for antibody levels to go down after acute infection, but they don’t go down to zero; they plateau. Here, we found antibody-producing cells in people 11 months after first symptoms. These cells will live and produce antibodies for the rest of people’s lives. That’s strong evidence for long-lasting immunity.
In another scientific publication that tackles the same myth, a June 2021 paper in the journal Nature explains that long-term immunity:
is not a long-lasting version of the immediate immune reaction to a particular virus; rather, it is a distinct aspect of the immune system. In the memory phase of an immune response, B and T cells that are specific for a virus are maintained in a state of dormancy, but are poised to spring into action if they encounter the virus again or a vaccine that represents it.
With specific regard to Fauci’s claim that weak antibody responses may be why immunity to the common cold doesn’t last, a December 2020 paper in the journal Vaccine X and a January 2021 paper in the journal Science explain that:
- “there are significant concerns about using antibody response in coronavirus infections as a sole metric of protective immunity.”
- “strong antibody response correlates with more severe clinical disease while T-cell response is correlated with less severe disease.”
- “the proportion of subjects positive for CD4+ T cells (92%) remained high at 6 to 8 months after infection.”
- B cells “were detected in almost all Covid-19 cases, with no apparent half-life at 5 to 8 months post-infection.”
In summary, the claims of media outlets and government agencies about naturally acquired immunity to Covid-19 are often at direct odds with the facts of this issue. Whether intended or not, this misinformation allows them to repeatedly blame variants for an ongoing tide of C-19 deaths despite more than 20 months of employing their remedies, such as lockdowns, social distancing, masking, and vaccines.
Unlike naturally acquired immunity to Covid-19, the immunity conferred by the current crop of C-19 vaccines seems to fade significantly within about six months. The evidence for this includes but is not limited to:
- a study released by Moderna.
- a study conducted by the CDC.
- a study conducted for the Department of Defense.
- a study conducted in Israel and published by the New England Journal of Medicine.
- a massive Pfizer-funded study published by The Lancet.
Contrary to the notion that mutations are the primary reason for the apparent decline in vaccine efficacy, the empirical evidence suggests that the vaccines work well against Delta and earlier variants, at least at the outset:
- A study published by the New England Journal of Medicine in July 2021 found that the Pfizer vaccine was about 93.7% effective against the Alpha variant and about 88.0% effective against the Delta variant.
- A study released by Moderna in September 2021 found that its vaccine was at first “highly effective against Covid-19” in a “real-world effectiveness study during” a “surge in Delta cases,” but this effectiveness fell considerably as time passed.
- A study published by The Lancet in October 2021 found that the Pfizer vaccine has “high effectiveness” in preventing “hospital admissions up until around 6 months after being fully vaccinated, even in the face of widespread dissemination of the Delta variant. Reduction in vaccine effectiveness against SARS-CoV-2 infections over time is probably primarily due to waning immunity with time rather than the Delta variant escaping vaccine protection.”
- A study published by the New England Journal of Medicine in October 2021 found that during a period of Delta variant dominance in Israel, the efficacy of the Pfizer vaccine in preventing Covid-19 was 80–83% for all age groups who were vaccinated two months earlier. This effectiveness fell for every month further back in time that people were vaccinated, dropping to 55–57% for those vaccinated six months earlier. The same study found that rates of severe C-19 among fully vaccinated people over the age of 40 were about twice as high for people who were vaccinated six months earlier than those who were vaccinated three months earlier.
Again, it is important to note that none of the studies above are randomized controlled trials, and thus, they are not conclusive. This lack of certainty exists because Pfizer, Moderna, and other vaccine manufacturers prematurely ended their randomized controlled trials in defiance of guidance issued by the International Coalition of Medicines Regulatory Authorities (ICMRA).
The ICMRA—a global association of 24 healthcare regulatory agencies including the FDA and its counterparts in Canada, Australia, China, France, Mexico, Japan, Nigeria, India, and other nations—declared in November 2020 that placebo-controlled randomized controlled trials for C-19 vaccines “should proceed as initially planned with a follow-up of at least one year or more from completion of assigned doses.” However, vaccine manufactures directly flouted those guidelines, leading the journal BMJ Evidence-Based Medicine to report in August 2021 that:
placebo controlled follow-up, originally planned for 2 years in many trials, was eliminated after a few months, when manufacturers began offering vaccine to placebo recipients within weeks of receiving emergency use authorisations.
Regardless, there is 100% certainty that enormous numbers of fully vaccinated people are now dying of Covid-19, something said to be impossible only six months ago. For example, on June 24, 2021—less than a week before the first clear evidence of widespread C-19 infections in fully vaccinated people became public—President Biden invoked the authority of Dr. Anthony Fauci in a prepared speech in which he stated:
Over 150 million Americans have gotten fully vaccinated and they’re safe and protected now, including against the Delta variant. … The data couldn’t be clearer: If you’re vaccinated—if you’re vaccinated, you’re safe.
Similarly, the New York Times reported on July 22, 2021 that even “as the Delta variant surges across the United States”:
“The takeaway message remains, if you’re vaccinated, you are protected,” said Dr. Celine Gounder, an infectious disease specialist at Bellevue Hospital Center in New York. “You are not going to end up with severe disease, hospitalization or death.”
For a staggering example of just how detached from reality those claims have proven to be, comprehensive data from the United Kingdom shows that 74% of all deaths involving Covid-19 from September 20 to December 12, 2021 were among the fully vaccinated. As the agency explains:
it is expected that a large proportion of cases, hospitalisations and deaths would occur in vaccinated individuals, simply because a larger proportion of the population are vaccinated than unvaccinated and no vaccine is 100% effective. This is especially true because vaccination has been prioritised in individuals who are more susceptible or more at risk of severe disease.
Despite the above and other facts that prove fully vaccinated people are dying in droves from Covid-19, media outlets and government officials are pushing the mantra “pandemic of the unvaccinated.” They do this with deceitful statistics that count all C-19 deaths among people “with unknown vaccination status” as people who are “not fully vaccinated.”
That crafty methodology is especially misleading in the U.S. where the CDC has warned that data on the vaccination status of people with Covid-19 “relies on passive and voluntary reporting, and data are not complete or representative.” Unscrupulous researchers can’t use this ruse with data from the UK because the government keeps detailed healthcare records of nearly all citizens. Moreover, the government openly counts C-19 deaths among the tiny portion of people with unknown vaccination status by labeling them as “Unlinked” to the nation’s vaccine registry.
Such grave disinformation prompted widely published medical scholar Günter Kampf to write letters published by medical journals documenting “increasing evidence that vaccinated individuals continue to have a relevant role in transmission” and why it is “wrong and dangerous to speak of a pandemic of the unvaccinated.”
The exact reasons why current Covid-19 vaccines have failed to protect so many people are not yet proven, but three possibilities rooted in empirical evidence (documented below) include the following:
- The vaccines are injected into muscles, which produces little-to-no immunity in the upper respiratory tract. In contrast, naturally acquired immunity produces robust immunity in both the upper and lower respiratory tracts.
- The vaccines target only one area of the virus called the “Spike protein,” while naturally acquired immunity targets the entire virus.
- The vaccines trigger an immune reaction to a few Spike variants, while naturally acquired immunity attacks a diverse array of Spike variants.
After explaining the second issue in the list above, a December 2020 paper in the journal Vaccine X warned “it would be a public health and general trust-in-medicine nightmare—including a boost to anti-vaccine forces—if immune protection wears off or new disease patterns develop among the immunized.”
The best available evidence indicates that the first element of that nightmare has come to pass. Definitive proof, however, is lacking because vaccine manufacturers closed down their main randomized controlled trials, thus preventing the collection of “gold standard” data beyond six months.
Among more than 180 Covid-19 vaccines that were in development by the fall of 2020, the FDA has fully approved one of them (Pfizer/BioNTech) and issued emergency use approvals for only two of them (Moderna and J&J/Janssen). Thus, the ensuing facts about the problems of Covid-19 vaccines apply only to these three products.
Problem 1: The Vaccines Don’t Protect the Upper Respiratory Tract
One of the primary defects of Covid-19 vaccines is that they generate almost no immunity in the nose, mouth, and other organs of the upper respiratory tract. This is where SARS-CoV-2 and other respiratory viruses enter the human body and first establish infections.
The underlying reason for this flaw is because Covid-19 vaccines are injected into muscles, which creates a different type of immunity than what occurs in the mucous membranes that line the upper respiratory tract. Spelling out the details of this reality, a September 2020 paper in the journal Nature about “SARS-CoV-2 vaccines in development” explains:
- “is important to note that natural infection” with respiratory viruses triggers the body to simultaneously produce two very different types of antibodies:
- “IgA” (immunoglobulin A), which appears in mucous that lines the nasal passages.
- “IgG” (immunoglobulin G) which appears in blood and tissues like the lung.
- this double immune response generated by natural infection “can lead to sterilizing immunity for many respiratory viruses.”
- “all of the vaccine candidates that are currently in clinical trials are administered intramuscularly,” or by injection into a muscle.
- injecting a vaccine into a muscle can trigger “strong IgG responses that are thought to protect the lower respiratory tract,” but “unlike natural infection it does not drive the secretory IgA responses that are thought to protect the upper respiratory tract.”
- “a vaccine that could induce sterilizing immunity in the upper respiratory tract would be preferable.”
- a narrow focus on developing intramuscular vaccines “could lead to vaccines that, although protecting from symptomatic disease, might still enable transmission of the virus.”
- a vaccine administered via a nasal spray or powder “would probably also lead to a strong mucosal immune response as well as an IgG response,” but “very few vaccines that are suitable for intranasal administration are undergoing development, and none are currently in clinical trials.”
Although media outlets have been virtually silent about those critically important facts, a range of medical journals have confirmed them, such as:
- a 2002 paper in the Journal of Infectious Diseases, which documents that:
- “the lower and upper respiratory tract differ in their mechanisms of immunity.”
- “many” of the “pathogens” that cause contagious respiratory diseases “infect the upper respiratory tract (nasal passages) prior to dissemination to the lower respiratory tract (airways and lungs).”
- “the generation of immunity against upper respiratory tract infections will decrease the chance of subsequent lower respiratory tract disease.”
- these facts “should be considered in vaccine development against” pneumonia-causing respiratory pathogens.
- a 2004 paper in the Journal of Immunology, which documents that:
- the “upper and lower respiratory tracts are immunologically separate in their response toward an infectious agent.”
- “the upper respiratory tract is the initial and major site of Ab [antibody] production after” infection with a pneumonia-causing microbe called “mycoplasma,” and “a similar phenomenon has been shown for other infectious agents.”
- “the lung is protected from mycoplasma infection by nasal-pulmonary or by systemic immunization” in a muscle, “while the nasal passages are protected only by certain “nasal immunizations.”
- a 2020 paper in the journal Infection and Immunity, which documents that:
- “there is a fundamental difference in immune and inflammatory responses generated in the upper and lower respiratory tracts.”
- “the upper respiratory tract is both the initial site of infection and the major locale for antibody” production after respiratory infections.
- the “optimal approach” for disease prevention to generate immune “responses in both the upper and lower respiratory tracts.”
- “generating immunity against upper respiratory tract infections will decrease the chance of subsequent lower respiratory tract disease.”
- “nasal immunization is an optimal approach to generate immunity throughout the respiratory tract.”
- “despite the promise of nasal immunization, there is also the potential to develop adverse” reactions to such vaccines.
- “approaches need to be developed to avoid potentially serious immunologic or inflammatory reactions” to nasal vaccines.
- a 2021 paper in the journal Drug Discovery Today, which documents that:
- “unlike conventional Coronavirus 2019 (Covid-19) vaccines, intranasal vaccines display a superior advantage because the nasal mucosa is often the initial site of infection.”
- “preclinical and clinical studies concerning intranasal immunization elicit high neutralizing antibody generation and mucosal IgA and T cell responses that avoid severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in both; the upper and lower respiratory tract.”
In short, the current Covid-19 vaccines do little-to-nothing to protect people’s upper respiratory tracts, which is where the SARS-CoV-2 virus first attacks them.
Problem 2: The Vaccines Only Target the Spike
Unlike other vaccines that provide long-lasting protection against diseases like polio and the measles, C-19 vaccines don’t prime your immune system to attack the entire virus that causes the disease. Instead, they target only one part of the virus called “the Spike protein,” or “Spike” for short, and “S” for shorter.
As its name suggests, Spike forms the physical spikes that appear on the exterior of coronaviruses and give them their signature look. This feature allows the viruses to latch onto and penetrate human cells.
Per a September 2020 paper in the journal Nature, C-19 vaccine developers focused on Spike because:
- it is the “one large surface protein” in “most coronaviruses.”
- antibodies that target Spike “prevent its attachment to the host cell and neutralize the virus.”
- the results of “preclinical studies” from other coronavirus vaccines showed that Spike was a good “antigenic target,” meaning that human immune cells aggressively attack it.
- they created the vaccines with “unprecedented speed” as compared to “traditional vaccine development,” which “can take 15 years or more.”
Similarly, a February 2020 paper in the journal Vaccines notes that “mRNA-based vaccines [like Pfizer and Moderna] have become an increasingly attractive platform to fight the ongoing SARS-CoV-2 pandemic for a multitude of reasons,” the first of which is “an exceedingly fast manufacturing timeline.”
While Spike-based vaccines can be quickly produced, they trigger a narrow immune response because they only attack one part of the virus. Medical journals like the following have documented the causes and implications of this fact:
- A study published in June 2020 by the journal Cell found that only 27% of the immune CD4+ T cell responses in people infected with SARS-CoV-2 targeted Spike, which was “somewhat unexpected” because data from 27 studies of other coronaviruses showed that “Spike accounted for nearly two-thirds of reported CD4+ T cell reactivity.” In other words, Spike in SARS-CoV-2 is not nearly as good of an “antigenic target” as assumed based on studies of similar viruses.
- A December 2020 paper in the journal Vaccine X reported that:
- “most vaccine candidates are focusing on Spike,” but the areas of SARS-CoV-2 that are targeted by the human immune system “are much less dominated by Spike protein than in previous coronavirus infections.”
- “natural infection by SARS-CoV-2 induces broad” immune responses against many other areas of the virus and even other types of coronaviruses.
- An “in-depth longitudinal study” of Covid-19 patients published by journal Cell Reports Medicine in July 2021 found that their “immune response to natural infection is likely to provide some degree of protective immunity against SARS-CoV-2 variants because” their T cells attack non-Spike areas of the virus that are not prone to mutate. Thus, the authors conclude that the vaccines might “benefit” from targeting those areas “rather than just to SARS-CoV-2 spike.”
- Another study also published in July 2021 by the journal Cell Reports Medicine found that:
- the “mutations of greatest concern” in SARS-CoV-2 variants are present in the viral spike (S) protein,” including several areas of it.
- the mutations of greatest concern “do not significantly disrupt the total CD4+ and CD8+ T cell responses” created by natural infection because they target many areas of the virus besides Spike.
- vaccines could provide “broader protective immunity against” variants and “minimize Covid-19 morbidity and mortality” if they targeted areas of the virus with “low mutational propensity,” like naturally acquired immunity.
A primary author of the study above, Ph.D. immunologist Dr. Rafi Ahmed, summarized its findings with these words:
- “Vaccines that target other parts of the virus rather than just the spike protein may be more helpful in containing infection as SARS-CoV-2 variants overtake the prevailing strains.”
- “This could pave the way for us to design vaccines that address multiple coronaviruses.”
This means that a single well-designed vaccine might provide immunity to all Covid-19 variants and even to other types of coronaviruses. Like numerous other facts above, this suggests that the real issue is the flaws of current vaccines, not the variants.
Even Fauci and company, who have relentlessly promoted the current Covid-19 vaccines, recently confessed in the New England Journal of Medicine:
The limitations of SARS-CoV-2 vaccines suggest that they will ultimately need to be replaced by second-generation vaccines that induce more broadly protective and more durable immunity.
A Google search reveals a total of zero national media outlets that have reported Fauci’s admission.
Problem 3: The Vaccines Target Very Few Spike Variants
Beyond neglecting to target any part of the SARS-CoV-2 virus besides the Spike protein, C-19 vaccines only target a genetically narrow range of Spike. For instance, the FDA’s approval summary for Pfizer’s C-19 vaccine boasts that the RNA it uses to trigger Spike production “contains two proline [protein] mutations” to create an “antigenically optimal” immune response. That is trifling compared to the diversity of Spike antigens produced by naturally acquired immunity:
- A June 2021 paper in the Proceedings of the National Academy of Sciences estimates that:
- “each infected person carries an estimated 1 billion to 100 billion” SARS-CoV-2 “virions during peak infection.”
- “the genetic diversity of virions in an infected host covers all possible single nucleotide substitutions,” a common form of mutations.
- the virions present in each person with Covid-19 “even cover a significant fraction of the possible pairs” of such mutations.
- An August 2021 paper in the journal Science reports that vaccines designed for protection against “the original” SARS-CoV-2 virus had “decreased … antibody responses” to Spike in the Alpha, Beta, Gamma, and Delta variants, while this was not the case for people with naturally acquired immunity to the original virus. Thus, the authors conclude that:
- vaccines should be developed “that increase the breadth and potency of antibodies” that target Spike.
- the “investigation of antibody responses” from people with naturally acquired immunity “can inform improvements to vaccine design and therapeutics.”
- A study published by the journal Nature in October 2021 found that the long-term immune B cells that people naturally generate from SARS-CoV-2 infections produce “memory antibodies” that “have greater potency and breadth” against Spike “than antibodies elicited by vaccination.”
All of these facts about the shortcomings of C-19 vaccines are consistent with the evidence that they initially provide strong protection against a wide range of variants, but this protection fades dramatically against the very same variants within six months. This accords with a July 2021 paper in the journal Open Forum Infectious Diseases, which explains that even when a variant causes “a significant increase in resistance” to specific immune cells, the activity of all the body’s immune cells can still be “high enough to confer complete protection.”
Such high levels of immune activity are the norm in the immediate wake of any infection or vaccination because antibodies are abundant, but these antibody levels drop substantially over the next six months because they are a short-term aspect of the immune system. This decline does not normally threaten long-term immunity because B cells and T cells confer protection, but these falling antibody levels can undercut the efficacy of vaccines that are poorly designed to elicit broad immune responses.
The same patterns are evident in preliminary data on Omicron, and the same people are misrepresenting and obscuring the data in ways that cover for the failures of their policies and actions.
Studies on the Omicron variant and C-19 booster shots are sparse and uncertain due to small datasets, a lack of peer-review due to time constraints, and the absence of “gold standard” randomized controlled trials because vaccine manufacturers terminated them. This means that all of them should be taken with a grain of salt.
Nevertheless, media outlets and politicians are spinning these tentative studies in ways that can harm or kill people. For a prime example, on the morning of December 8, 2021, the New York Times published a “Covid Live Update” with the title:
Blood samples of people who received two Pfizer doses showed a 25-fold reduction in antibody levels against Omicron
Given that people with two doses of Pfizer’s vaccine are considered by the CDC to be fully vaccinated, this sounds like a stunning failure of the product. Yet, the Times publicized and linked to the update by placing the following headline at the top of its home page:
Pfizer-BioNTech Says Booster Offers Significant Protection Against Omicron
And less than an hour later, the Times changed the title of the update to read, “Pfizer says its boosters protect against Omicron.” The Times also inserted a quote from President Biden calling these findings “very, very encouraging” and declaring, “If you get the booster, you’re really in good shape.”
Later that day, the Times packaged the same basic content into an article and added the phrase “Strong Protection” to its title.
All of those glowing headlines and Biden’s statement are based on a Pfizer press release containing information that is far less optimistic than Biden and the Times lead people to believe. In it, Pfizer reveals that the blood tests were performed only on the “Spike protein” and that “these antibody levels” are merely “associated with high efficacy” against earlier variants, not that they provide “Strong Protection” against Omicron.
Most importantly—yet absent from the Times’ coverage and Pfizer’s press release—is the fact that the booster is the exact same formulation as the original vaccine. This raises the question of why a third dose of the very same RNA would produce a genetically different response from the two previous doses.
The results of broader studies indicate that it does not. One of these was recently published in a working paper, which means that, like the Pfizer study, it has not yet undergone peer review. But unlike Pfizer’s press release, the paper contains copious details and a file of supplementary data documenting the results. Moreover, it measures a very important factor that the Pfizer study ignores.
Without daring to risk a straightforward comparison of vaccination to naturally acquired immunity, the authors of the study compared antibody responses to Omicron in blood drawn from people who were vaccinated versus people who were both vaccinated and previously infected with an earlier SARS variant. They found that people who were both infected and vaccinated had exponentially higher antibody activity than people who were merely vaccinated.
Furthermore, the study was performed with blood samples drawn from people “soon after vaccination, so that vaccine elicited neutralization was close to peak.” The authors noted that their results are inconsistent with Pfizer’s Omicron booster study because “both groups had 22-fold Omicron escape from vaccine elicited neutralization.”
Those results accord with the following conclusion about boosters published in a July 2021 working paper but diplomatically reworded when published by the journal Nature in October 2021:
Boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing [antibody] activity but not the qualitative advantage against variants obtained by vaccinating convalescent [naturally infected] individuals.
Yet that is the path Fauci advocated in a White House press briefing on December 15 in which he stated, “And so, finally, our booster vaccine regimens work against Omicron. At this point, there is no need for a variant-specific booster.” The danger with this approach of ramping up the quantity to compensate for poor quality is that the side effects of Covid-19 vaccines tend to worsen with each dose.
For example, a study of 2,030 subjects published by the European Journal of Hospital Pharmacy in July 2021 found that:
- among people who were not previously infected with SARS-CoV-2:
- 29% experienced side effects after the first dose of the Pfizer vaccine.
- 71% experienced side effects after the second dose of the Pfizer vaccine.
- among people who were previously infected with SARS-CoV-2:
- 47% experienced side effects after the first dose of the Pfizer vaccine.
- 63% experienced side effects after the second dose of the Pfizer vaccine.
- “adverse reactions following immunization” were “generally more frequent and severe”:
- “in people under the age of 50.”
- “in females compared with males.”
- “these findings are in agreement with” two other studies which showed that “vaccine-associated systemic side effects are more common among younger people and after the second dose of the vaccine….”
Though most of the side effects were minor, they occurred on just the second dose (instead of a third booster dose), and the authors reported that:
- severe allergic reactions are “usually” uncommon “for most vaccines” and occur “at a rate of less than one per million doses,” but the rate for the Pfizer C-19 vaccine is “closer to” one in 125,000.
- even though their study “was conducted in a limited population” of 2,030 people, one subject experienced a “severe” reaction, “potentially due to an anaphylactic syndrome” although the “real” cause “remains unknown.”
Regarding the risks to children, Pfizer’s late October briefing document for the FDA details several adverse events from a tiny study of about 2,400 children with an average enrollment time of 2.2 months. Crucially, the study excluded children apt to have side effects from vaccines, like those with a “history of severe adverse reaction associated with a vaccine” and “individuals with a history of autoimmune disease or an active autoimmune disease.” Even still:
- “one participant withdrew” after the first dose because the child experienced:
- a “severe” fever that peaked at 104.2 ºF (40.1 °C) on the third day after the vaccine and subsided a day later.
- a marked decline in a type of white blood cells produced in bone marrow that are crucial to stopping bacterial infections. The girl had a “benign” medical history of this condition, but her levels dropped from 480/mm3 before the vaccine to 20 on the second day after the vaccine and then “improved to 70” by 23 days after the vaccine. Per the Gale Encyclopedia of Medicine, when levels of these cells decline below 200, “there is a “risk of overwhelming infection” which “requires hospital treatment with antibiotics.”
- another participant with “no reported medical history” of any conditions before the vaccine experienced these allegedly “non-related” adverse events after the first dose and did not take the second dose:
- “mild headache with onset at 10 days after Dose 1 and resolved in 2 days.”
- “mild joint swelling of the right ankle with onset at 16 days after Dose 1 and resolved in 3 days.”
- “mild Henoch-Schoenlein purpura with onset of 21 days after Dose 1 and reported as ongoing at the time of the data cutoff date.” Per the Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, this disease involves blood escaping into “tissues, under the skin, and through the mucous membranes,” and it “may be associated with exposure to drugs or other chemical agents, systemic diseases such as multiple myeloma and leukemia, diseases affecting the bone marrow or spleen, and infectious diseases such as rubella (German measles).”
And buried near the end of a long paragraph on the 68th page of the same briefing document, Pfizer reveals that “one fatality occurred” from a heart inflammation condition called myocarditis in “a study from Israel.” The study, published by the New England Journal of Medicine in October 2021, also found that the incidence of myocarditis among males aged 16 to 19:
- was 4–18 times greater in the fully vaccinated than in the unvaccinated.
- increased by 8–19 times between the first and second doses of the Pfizer vaccine.
Because immunocompromised and elderly people were prioritized for boosters, studies of third-dose side effects among young people with healthy immune systems are rare. This is concerning because a February 2021 paper in the World Allergy Organization Journal notes that:
- “the vast majority of adverse events following immunization are a consequence of the vaccine stimulating a protective immune response” instead of allergic reactions.
- “vaccines against Covid-19 are new and some (for example, the mRNA vaccines) have a novel mechanism of action; thus the risk of allergic reactions may be greater than for conventional vaccines.”
A working paper that presents the results of a small study of “168 non-immunocompromised” healthcare workers in Monterrey, Mexico found that “tiredness, myalgias [muscle pains], arthralgias [joint pains], fever, and adenopathy [swollen glands] were proportionally higher following the third dose than” either the first or second dose.
The study found “no severe side effects in the short-term,” and the authors note that “the third dose had less number of total side effects compared to the other two shots.” However, the bulk of those side effects were local like “pain at the injection site,” while more serious systemic reactions like fatigue, joint pain, and heart palpitations generally increased with each dose:

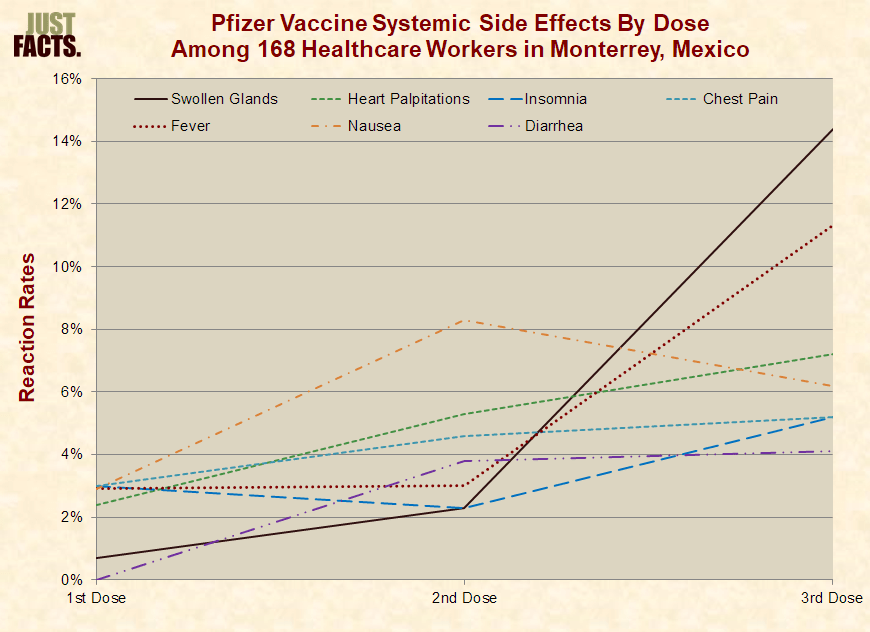
Not all of these differences are statistically significant due to the small size of the study, but this is a classic dose-response pattern. As explained by epidemiologist Sydney Pettygrove, a dose-response pattern “is considered strong evidence for a causal relationship between the exposure and the outcome.”
Worse still, it appears that the vaccines may only protect against becoming infected with Omicron for a single month. A nationwide study conducted in Denmark and reported in a December 2021 working paper found that:
- two doses of the Pfizer vaccine reduced the odds of becoming infected with Omicron by 24–74% among people who received the second dose in the previous month.
- this protection “declines rapidly” so that people who received the second dose only two months prior had no statistically significant protection.
- a third booster dose reduced the odds of becoming infected with Omicron by 30–70% for people who received the third dose in the previous 14 to 44 days.
- the Moderna vaccine had roughly the same numbers with higher margins of uncertainty due to smaller samples.
Based on those results, the authors declare, “In light of the exponential rise in Omicron cases, these findings highlight the need for massive rollout of vaccinations and booster vaccinations.” Hidden beneath that conclusion and never mentioned in the text of the paper is a chart and table showing that unvaccinated people were:
- 20–62% less likely to become infected with Omicron than those who received the second dose of the Moderna vaccine 4 to 5 months prior.
- 60–95% less likely to become infected with Omicron than those who received the second dose of the Pfizer vaccine 4 to 5 months prior.
All of this and more weighs against cavalierly getting repeated C-19 vaccinations to compensate for their inadequacies. This doesn’t mean that people shouldn’t get vaccinated or boosted. It means that they and their healthcare providers should apply this vital principle stated in plain language by the United Kingdom’s Medicines & Healthcare Products Regulatory Agency:
All vaccines and medicines have some side effects. These side effects need to be continuously balanced against the expected benefits in preventing illness.
Doing that requires broad and detailed knowledge about Covid-19, the vaccines, and each individual’s health status. And obtaining that requires deep, serious research because many politicians, commentators, media outlets, government agencies, pharmaceutical companies, so-called fact-checkers, and “experts” have repeatedly shown that they cannot be trusted.
Beyond failing to recognize the import of naturally acquired immunity and failing to design vaccines that replicate it, one of the deadliest blunders of the authorities responsible for C-19 policies is failing to protect highly vulnerable people from exposure to the virus. This has allowed the virus to ravage nursing homes, hospitals, and other places where their chosen mitigation measures have been used in spades.
The blame for this lies with the World Health Organization, the CDC, and other “experts” who denied the fact that C-19 is mainly transmitted by respiratory aerosols. These microscopic particles are light enough to stay airborne for minutes to hours and easily circumvent most masks, spittle barriers, and other measures claimed to block the spread of the virus. This is proven by at least 20 papers published in scientific journals showing that Covid-19 and all other contagious respiratory diseases are mainly spread by fine aerosols instead of large droplets.
Yet with complete disregard for the facts of this matter, WHO published a “fact check” in March 2020 insisting that “Covid-19 is NOT airborne” and “is mainly transmitted through droplets” that “are too heavy to hang in the air”:

Similar claims about “droplets” were widely propagated by the likes of the CDC, Holmes Lybrand of CNN, and Paul Krugman of the New York Times. This deadly falsehood was the party line for more than a year. Then over one week in the spring of 2021, both the CDC and WHO quietly changed their webpages on how Covid-19 transmits to admit that it can spread via “very small particles” and “aerosols.”
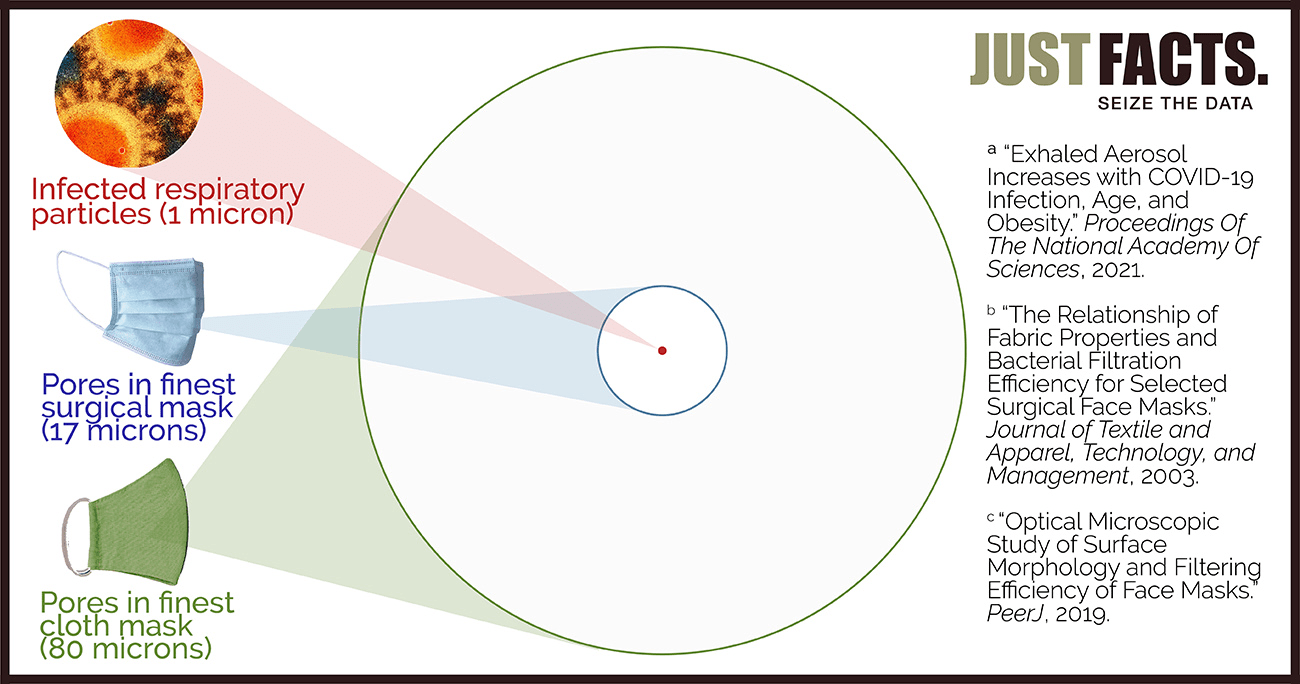
The implications of this are staggering because the vast bulk of these aerosols are less than 1 micron in diameter, which is 1/17th the size of the pores in the finest surgical masks and 1/80th the size of the pores in the finest cloth masks. These figures, which were routinely ignored by public health officials and the press, are documented in:
- a study published by the Proceedings of the National Academy of Sciences in February 2021, which found that more than 90% of the virus-carrying aerosols exhaled by primates infected with C-19 are less than 1 micron in diameter.
- a study published in 2003 by the Journal of Textile and Apparel, Technology, and Management, which analyzed six types of surgical masks and found that their average pore sizes ranged from 17 to 51 microns
- a study published in 2019 by the journal PeerJ, which analyzed 20 types of cloth masks and found that their pore sizes ranged from 80 to 500 microns.
Yet instead of candidly announcing they were wrong about this life-or-death issue, the CDC and WHO nonchalantly changed their webpages as if it had no import. However, epidemiologists knew full well that it had fatal consequences.
To wit, Mary-Louise McLaws, an epidemiologist and member of WHO’s Covid-19 infection control committee, told the New York Times in July 2020 that she was “frustrated” by WHO’s stubbornness on the issue of aerosols and wanted them to revisit this issue. She emphasized that a change in WHO’s position “will cause an enormous shudder through the infection control society” and that “we would have to be prepared to change a lot of what we do.”
The CDC clearly knew that—for on the same day that it changed its webpage on how C-19 spreads—it deleted from the webpage a statement which reveals the harm caused by their misinformation. Explaining what must change if C-19 were airborne, it stated: “Pathogens that are spread easily through airborne transmission require the use of special engineering controls to prevent infections,” including highly ventilated rooms and fit-tested respirators. Ignorance of this fact buried by the CDC has allowed countless preventable deaths to continue to this day.
Extensive details about this issue are available in Just Facts’ research on masks, but the bottom line is that the most effective way to stop the spread of infectious respiratory aerosols is to kill the microbes instead of trying to block or contain them. One affordable engineering control that has proven particularly effective is ultraviolet air disinfection.
In light of Omicron, which appears to be far more contagious than earlier variants, these facts warrant more attention than ever. The same applies to this next topic.
Another catastrophic misstep in the battle against C-19 has been locking down healthy children and young adults who are far more likely to die from the common hazards of life than from Covid. This has caused tremendous harm for little benefit, and the tradeoffs look even worse for Omicron.
Since the outset of the pandemic on March 11, 2020 through October 2, 2021, 1% of all deaths of U.S. children under the age of 18 involved C-19. Among 18–29 year olds, this figure is 3%, rising to 13% for people aged 65 and older. Per the CDC, these figures include all deaths “involving” Covid-19.
One of the few, if not the only, credible study of children who have “died from” Covid-19 as opposed to “those who died of an alternative cause but coincidentally tested positive” for C-19 appears in a July 2021 working paper by the UK National Child Mortality Database. The study found that during the first year of the pandemic in England, C-19 took the lives of one out every 500,000 children under the age of 18.
For comparison, children in the U.S. under the age of 18 are five times more likely to die of drowning and 36 times more likely to die of accidents.
C-19 deaths among healthy people also pale in lethality to the unintended consequences of lockdowns. Some studies that have quantified this loss of life include the following:
- A study conducted in Switzerland and published by the journal European Psychiatry in May 2020 found that:
- governments failed to model the “increased short-term and long-term mortality” caused by the mental health impacts of Covid-19 mitigation strategies like social distancing and lockdowns.
- these actions increased “suicide, depression, alcohol use disorder, childhood trauma due to domestic violence, changes in marital status, and social isolation.”
- this harm will ultimately be “borne by 2.1% of the population, who will suffer an average of 9.79” years of life lost. In comparison, Covid-19 has killed about 0.2% of the U.S. population at an average age of 75 years.
- A study published in November 2020 by the journal JAMA Network Open estimated that decisions to close down elementary schools in the spring of 2020 will eventually shorten the lives of U.S. children aged 5–11 by 2.5–42.1 million years due to the effects of “decreased educational attainment.” In comparison, if a million people in the U.S. die from C-19, this will rob 13.2 million years of life from Americans of all ages.
- A study published in September 2021 by the International Journal of the Economics of Business estimated the harms and benefits of lockdowns in Canada and found that they destroy 141 years of life for every year of life saved.
Nor do lockdowns of healthy people necessarily protect the vulnerable from Covid-19. This is because lockdowns prevent the development of herd immunity, enabling C-19 to surge after lockdowns are ended. Even the Imperial College of London, which provided the impetus for mass lockdowns, admitted in March 2020 that the “more successful a strategy is at temporary suppression, the larger the later epidemic is predicted to be in the absence of vaccination, due to lesser build-up of herd immunity.”
In fact, locking down healthy people can actually increase C-19 transmission to unhealthy people. A study published by the British Medical Journal in October 2020 found these “counterintuitive results” about lockdowns in the United Kingdom:
- The advice given to UK policymakers was focused “on reducing total number of cases and not the number of deaths.”
- “Contrary to popular perception,” the Imperial College model that was used to justify the lockdown never “specifically modelled” the lockdown.
- When adjusted to reflect high transmissibility of C-19, the Imperial College model projects that once some basic preventative measures are in place like quarantining infected people and social distancing for the elderly:
- the “closure of schools and universities would increase the total number of deaths.”
- “general social distancing” of the entire population “was also projected to increase the total number of deaths.”
- “postponing the spread of Covid-19 means that more people are still infectious and are available to infect older age groups, of whom a much larger fraction then die.”
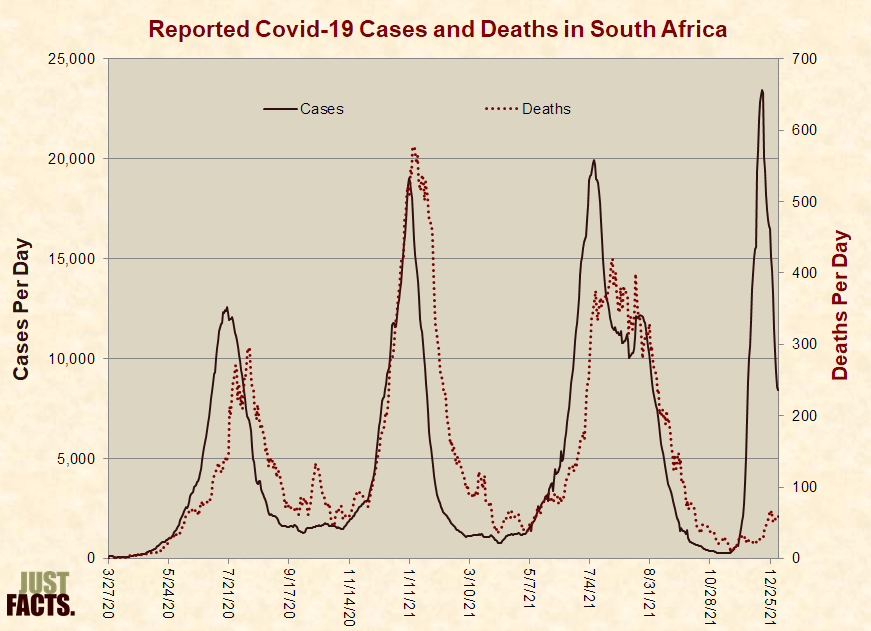
Such outcomes are natural consequence of the fact that C-19 has high transmissibility and a death rate of well under 1%. Omicron makes the dynamics of lockdowns even less favorable because the variant seems to be far more contagious and far less deadly to those who catch it. This is evidenced by early data from South Africa, one of the first large nations to experience a major outbreak of Omicron.
Throughout the pandemic, South Africa followed the typical pattern of surging C-19 cases followed by surging deaths—until the recent outbreak of Omicron. This caused a massive increase in reported cases with a small increase in deaths, a phenomenon known as “decoupling”:
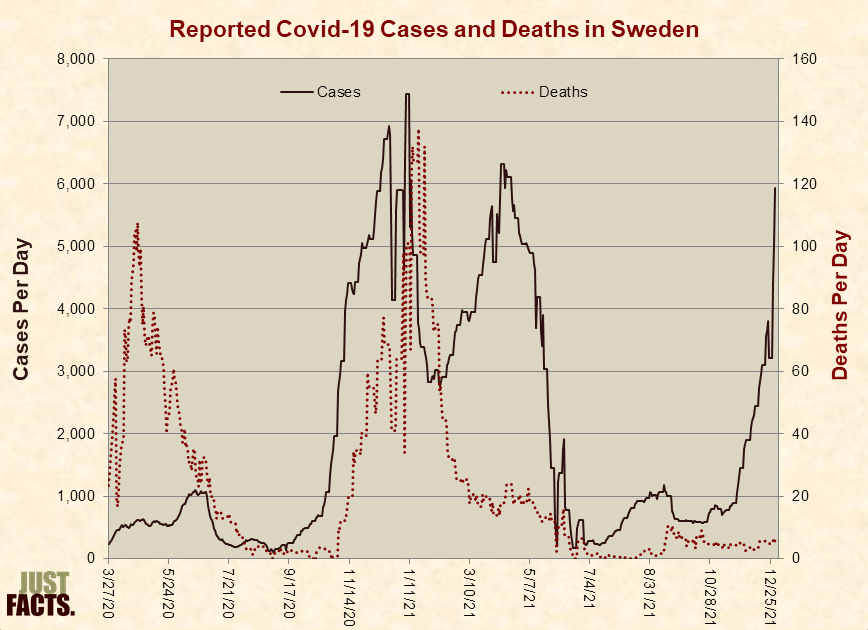
The pattern is even more unusual in Sweden, one of the few nations that shunned lockdowns and built widespread natural immunity. In Sweden, decoupling began near the outset of 2021, and deaths have stayed low throughout the Delta wave and into the early stages of Omicron:
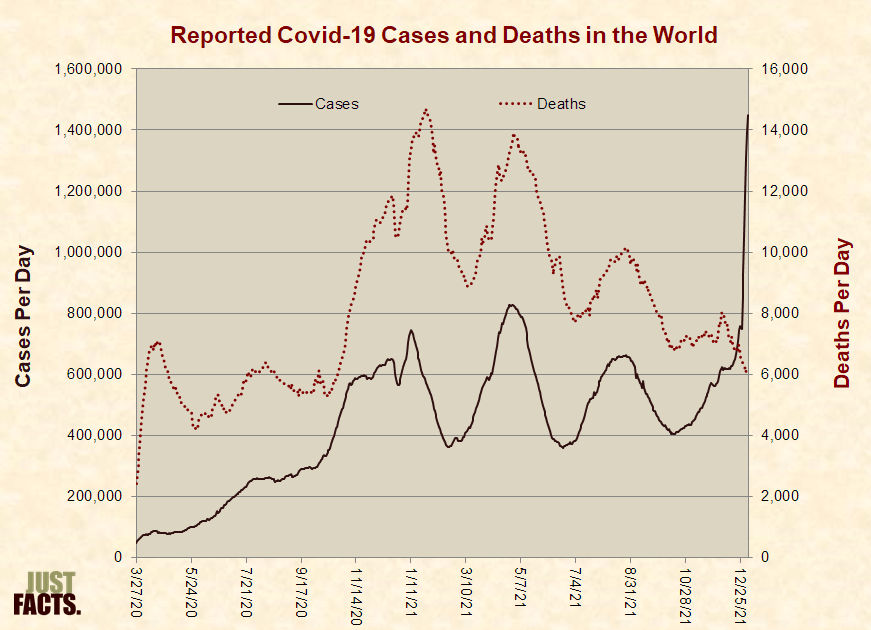
And for the first time in the history of the pandemic, a decoupling appears to have begun on a worldwide basis, although it is still too soon to be certain:
All of the facts above suggest that locking down for Omicron will be even more counterproductive than earlier lockdowns. Yet, that is what certain public officials are doing now, such as these:
- Prime Minister Mark Rutte of the Netherlands—where 86% of people over the age of 17 are fully vaccinated—recently shut down all schools and businesses except those that provide basic needs. He also prohibited people from having more than two guests in their homes and being together outside in groups of more than two.
- The decisionmakers who run more than 3,000 schools throughout the U.S. have temporarily cancelled classes and switched to remote teaching in places like Newark (NJ), Detroit (MI), and St. Louis (MO).
- Authorities in Quebec, Canada have shut down all “schools, bars, gyms and movie theatres,” mandated that all “non-essential workers” stay home, and ordered people to “limit your contacts to absolute minimum.”
Summary
Scores of rigorously documented facts show that politicians and public health officials have mishandled the Covid-19 pandemic in grossly negligent ways that have harmed and killed countless people. With cover from the media, this cabal is blaming the Omicron and Delta variants for the devastation caused by their actions.































This website is now targeted for extinction by the Fauci/Biden Regime.
Have a nice day, and next time you decide to speak get your statements pre-approved by The Ministry of Truth.
What if you offer FAKE local news stations money to find flaws in your article ?
After all with so many “Experts” that are NEVER WRONG, that should be easy for them.
What do readers think is the real explaination why people in power don’t even want to debate the ideas listed in this article ?
A fourth potential reason for problems with vaccine-induced immunity is that it is in effect acting to select out resistant variants, much as antibiotic-resistant bacteria become selected for in arenas where high frequency of antibiotic usage occurs (like certain medical centres).